BRUKINSA TOLERABILITY vs OTHER BTKis1,2
Study 215 is an ongoing Phase 2 exploratory study in patients (N=92) with B-cell malignancies who were intolerant to acalabrutinib or ibrutinib, leading to discontinuation. The following data are from a long-term update of only patients with CLL/SLL (n=71).*1,2
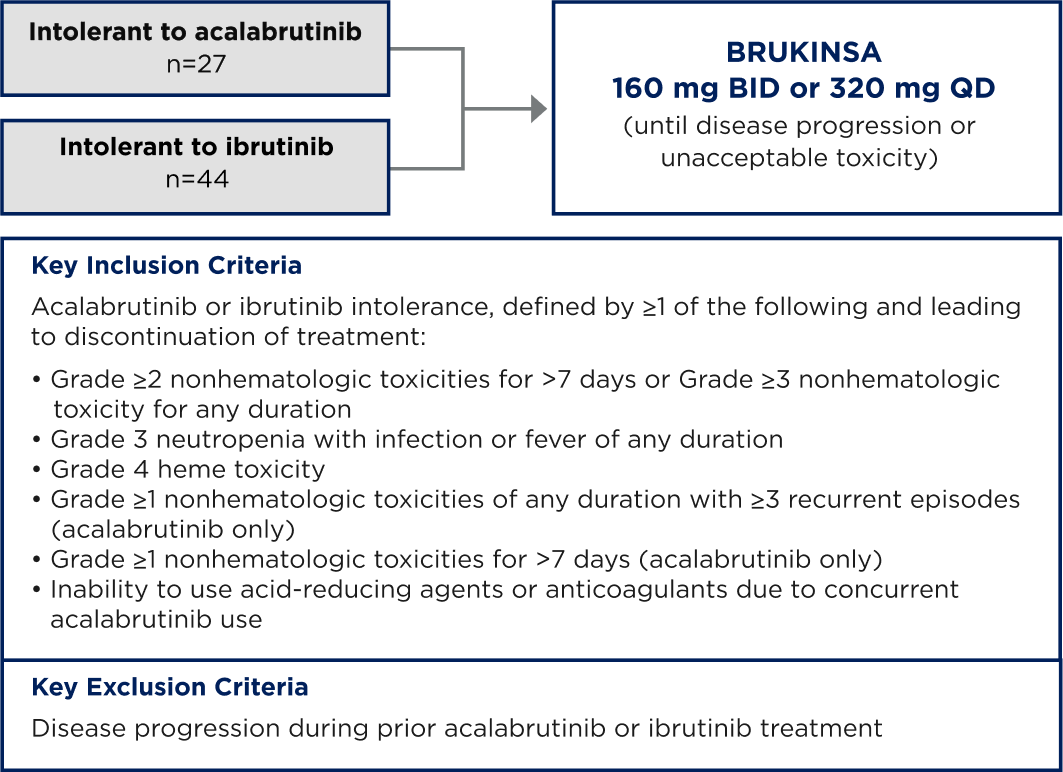
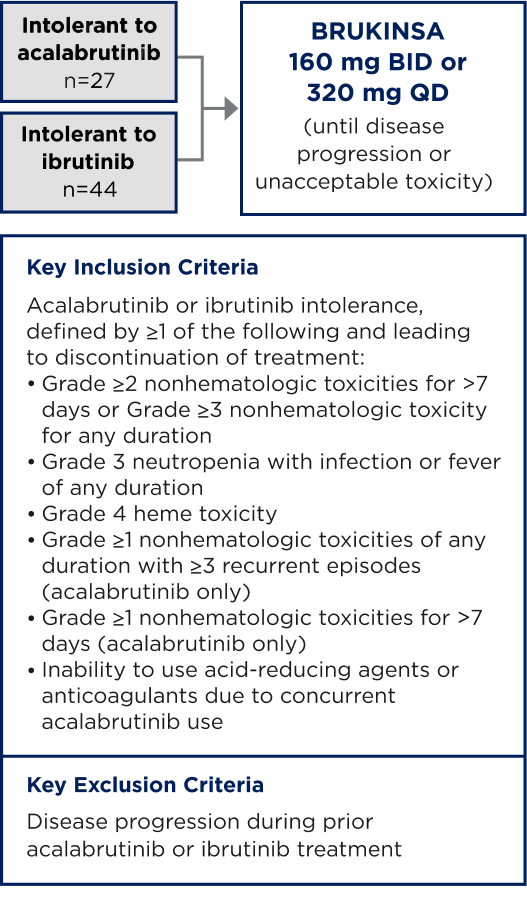
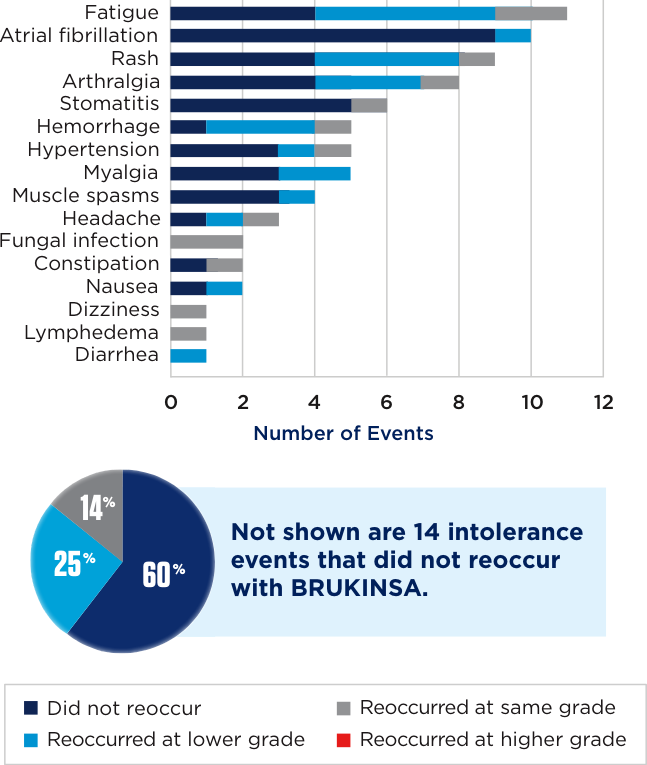
Primary endpoint: Recurrence and change in severity of acalabrutinib- and/or ibrutinib-intolerant events1
- AEs were collected retrospectively and evaluated and graded according to NCI CTCAE version 5.0. In patients with CLL, treatment-emergent cytopenias were graded per iWCLL criteria1
Select secondary endpoints: DCR, ORR, and PFS1
There are no head-to-head trials between BRUKINSA and acalabrutinib.
All data are descriptive in nature.
*Of the 27 patients who were intolerant to acalabrutinib, 17 were intolerant to acalabrutinib only, and 10 were intolerant to both ibrutinib and acalabrutinib.1
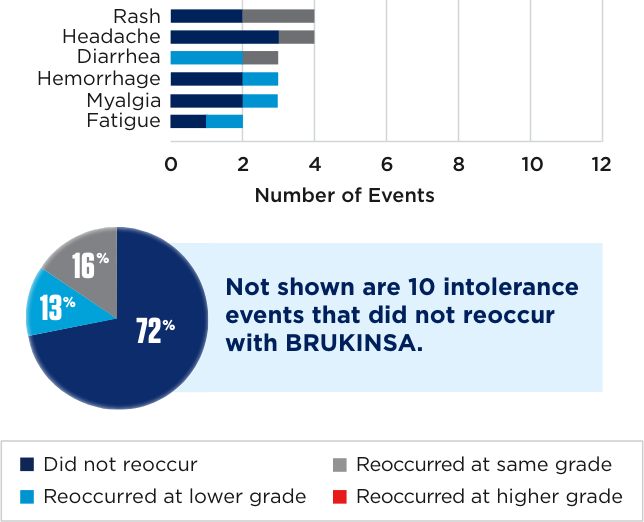
~TWO-THIRDS OF INTOLERANCE EVENTS THAT OCCURRED WITH ACALABRUTINIB OR IBRUTINIB DID NOT OCCUR AFTER PATIENTS STARTED BRUKINSA1

There are no head-to-head trials between BRUKINSA and acalabrutinib.
The most common AEs (≥20%) with BRUKINSA in acalabrutinib-intolerant patients were fatigue (30%), diarrhea (26%), hypertension (26%), and cough (22%).1
(primary endpoint)†1
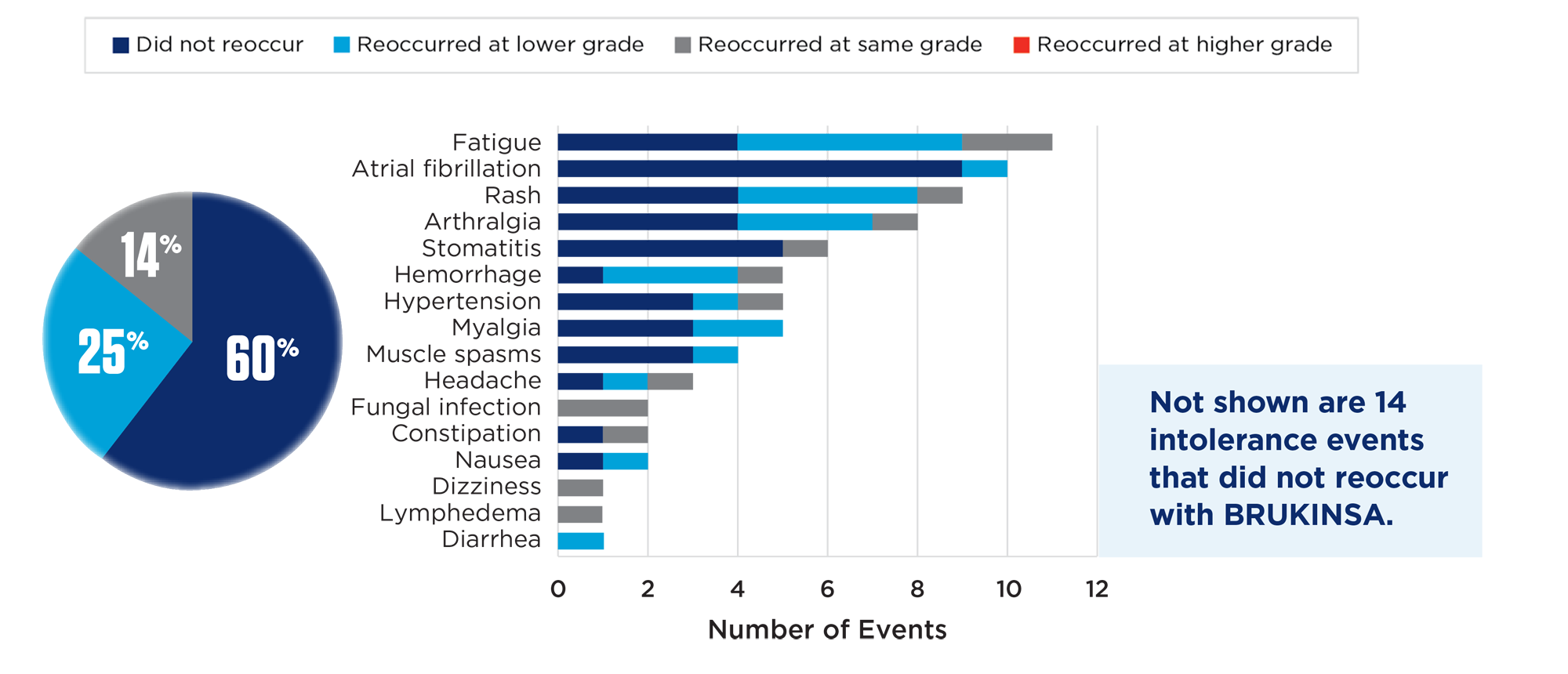
The most common AEs (≥20%) with BRUKINSA in ibrutinib-intolerant patients were fatigue (34%), COVID-19 (34%), contusion (27%), constipation (25%), diarrhea (23%), arthralgia (23%), cough (21%), upper respiratory tract infection (21%), nausea (21%), sinusitis (21%), and headache (21%).1
No AEs that occurred with acalabrutinib or ibrutinib occurred at a higher grade with BRUKINSA1
- 11% of patients treated with BRUKINSA discontinued treatment due to TEAEs1
Response rates maintained or improved with BRUKINSA1
All data are descriptive in nature.
Median follow-up for acalabrutinib-intolerant patients was 16.5 months with a data cutoff of May 1, 2024. Median follow-up for ibrutinib-intolerant patients was 41.8 months with a data cutoff of May 1, 2024.1
†Rounded rates do not total 100%.
‡Secondary endpoint; data are descriptive in nature.1
AEs=adverse events; BID=twice daily; BTKis=Bruton’s tyrosine kinase inhibitors; CLL=chronic lymphocytic leukemia; COVID-19=coronavirus disease 2019; DCR=disease control rate; iWCLL=International Workshop on Chronic Lymphocytic Leukemia; NCI CTCAE=National Cancer Institute Common Terminology Criteria for Adverse Events; ORR=overall response rate; PFS=progression-free survival; QD=once daily; SLL=small lymphocytic lymphoma; TEAEs=treatment-emergent adverse events.
References: 1. Shadman M, Burke JM, Cultrera J, et al. Zanubrutinib is well tolerated and effective in patients with CLL/SLL intolerant of ibrutinib/acalabrutinib: updated results. Blood Adv. 2025;9(16):4100-4110. 2. Shadman M, Flinn IW, Levy MY, et al. Zanubrutinib is well tolerated and effective in acalabrutinib-intolerant patients with B-cell malignancies. Presented at: American Society of Hematology (ASH) Annual Meeting and Exposition; December 7-10, 2024. Poster 4632.