BRUKINSA was designed to meet the challenges of BTK inhibition, including in adult patients with CLL2
SUPERIOR EFFICACY ACROSS LINES OF THERAPY2-4
CONSISTENT PFS FOR ALL CLL PATIENT SUBGROUPS STUDIED
Superior PFS vs BR in patients without del(17p) with consistent PFS in the largest prospective study of 1L patients with del(17p)2,4
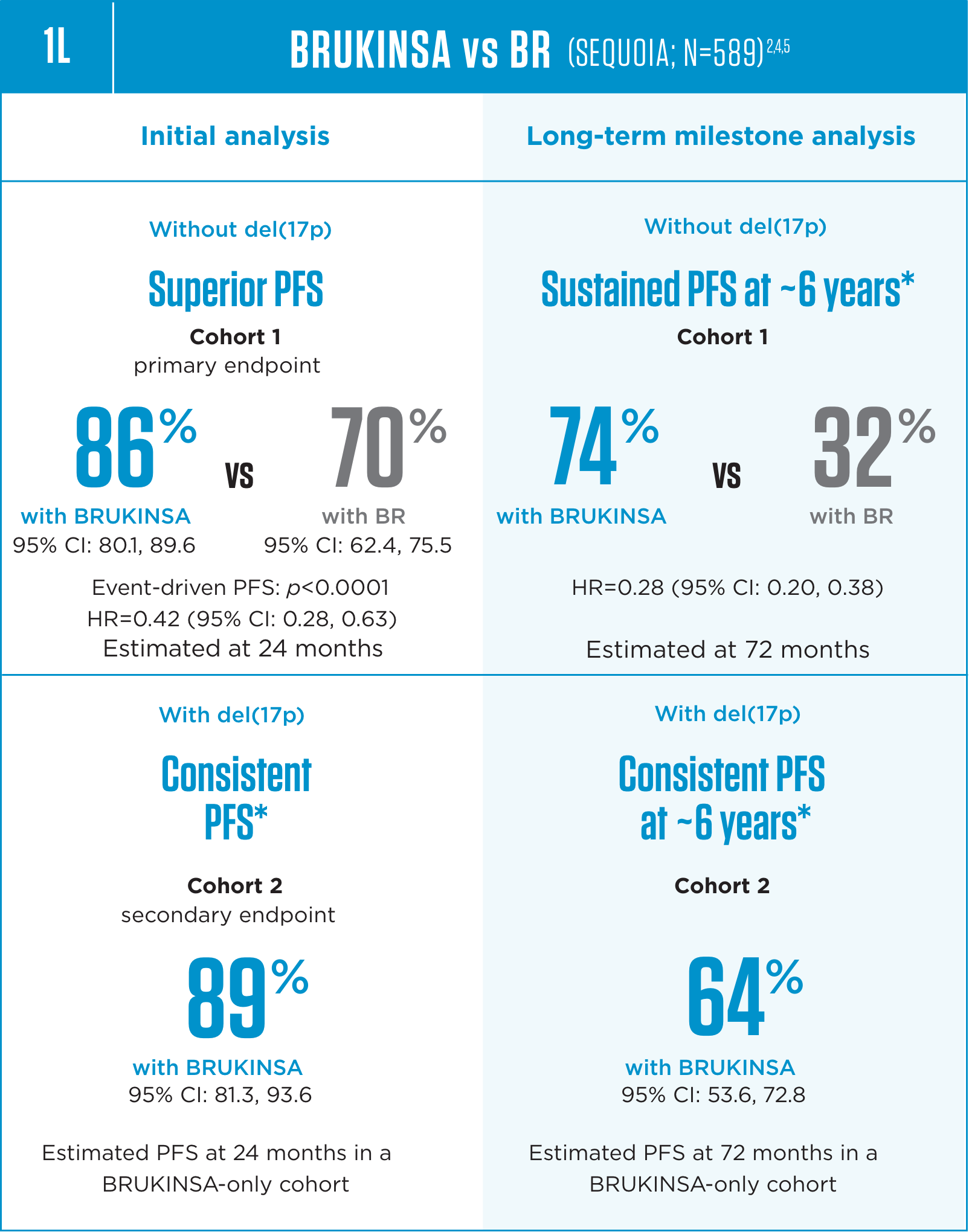
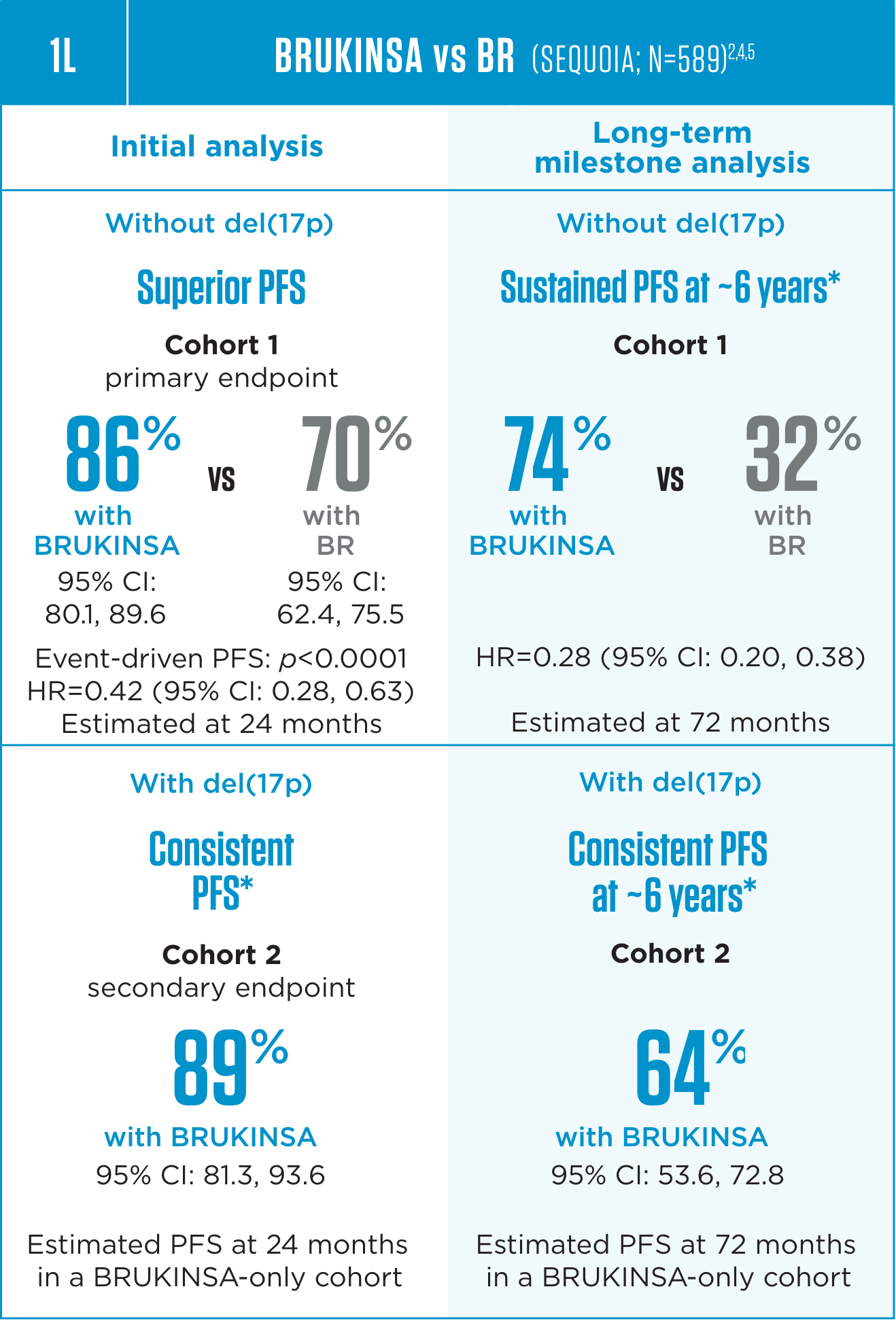
Median follow-up: 26.2 months for Cohort 1 and 30.5 months for Cohort 2 at the initial analysis; 72.8 months for Cohort 1 and 76.7 months for Cohort 2 at the long-term follow-ups.4,5
The only BTKi with superior
efficacy vs ibrutinib in 2L, regardless
of mutation status2,3
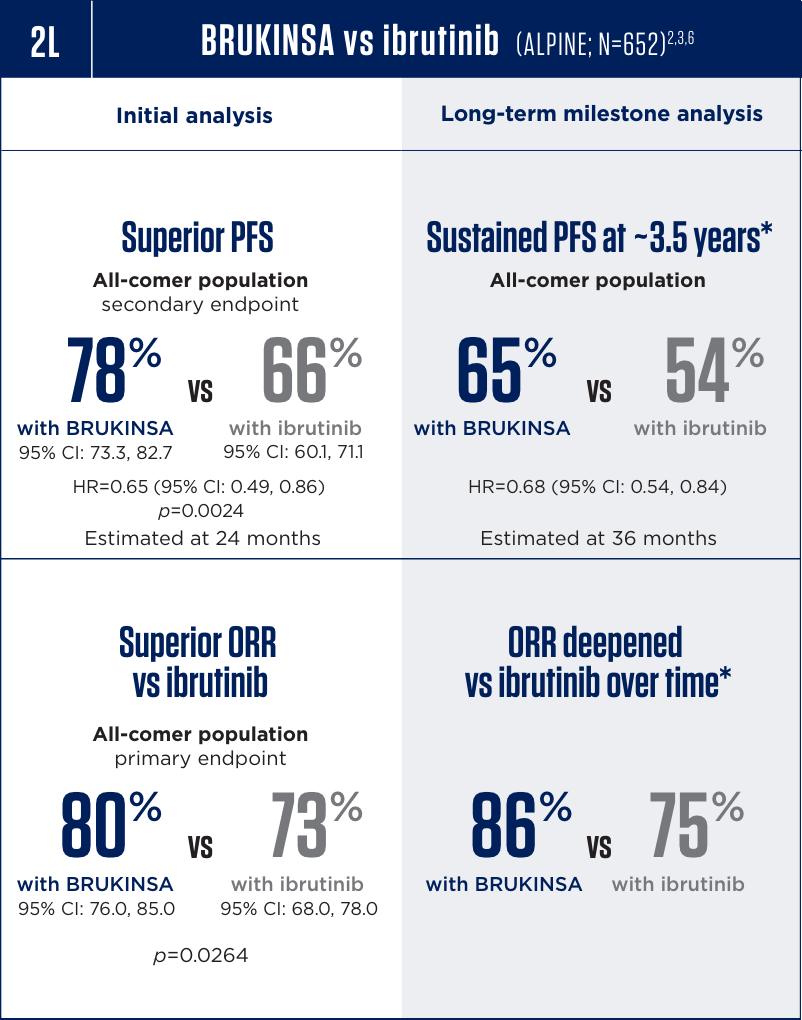
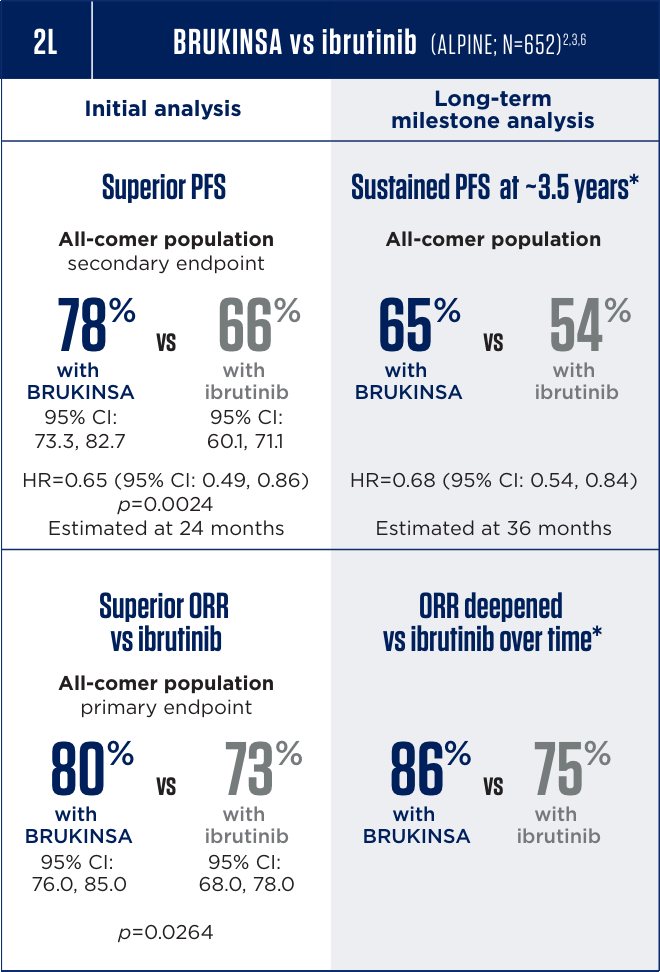
Median follow-up: 31 months for PFS and 24.7 months for ORR at the initial analysis; 42.5 months for PFS and ORR at the long-term follow-up.2,6,7
All analyses are exploratory and descriptive in nature.
SEQUOIA: global Phase 3, randomized, open-label, multicenter trial in treatment-naïve CLL/SLL. Cohort 1 (BRUKINSA vs BR; n=479): patients without del(17p). Cohort 2 (BRUKINSA only; n=110): patients with del(17p). Primary endpoint: PFS (IRC, ITT population). Superiority: 2-sided, α=0.05.2,4
ALPINE: global Phase 3, randomized, open-label, multicenter trial in R/R CLL/SLL (≥1 prior systemic therapy). BRUKINSA vs ibrutinib (N=652). Endpoints assessed for noninferiority: ORR (primary) and PFS (key secondary). Superiority tested when noninferiority was met.2,3
1L=first line; 2L=second line; BR=bendamustine+rituximab; BTK=Bruton’s tyrosine kinase; BTKi=Bruton’s tyrosine kinase inhibitor; CI=confidence interval; CLL=chronic lymphocytic leukemia; HR=hazard ratio; IRC=independent review committee; ITT=intent to treat; ORR=overall response rate; PFS=progression-free survival; R/R=relapsed/refractory; SLL=small lymphocytic lymphoma.
CONSISTENTLY LOW RATES OF AFIB/FLUTTER
AND DISCONTINUATION ACROSS TRIALS
CONSISTENCY IN 2 GLOBAL PHASE 3 TRIALS
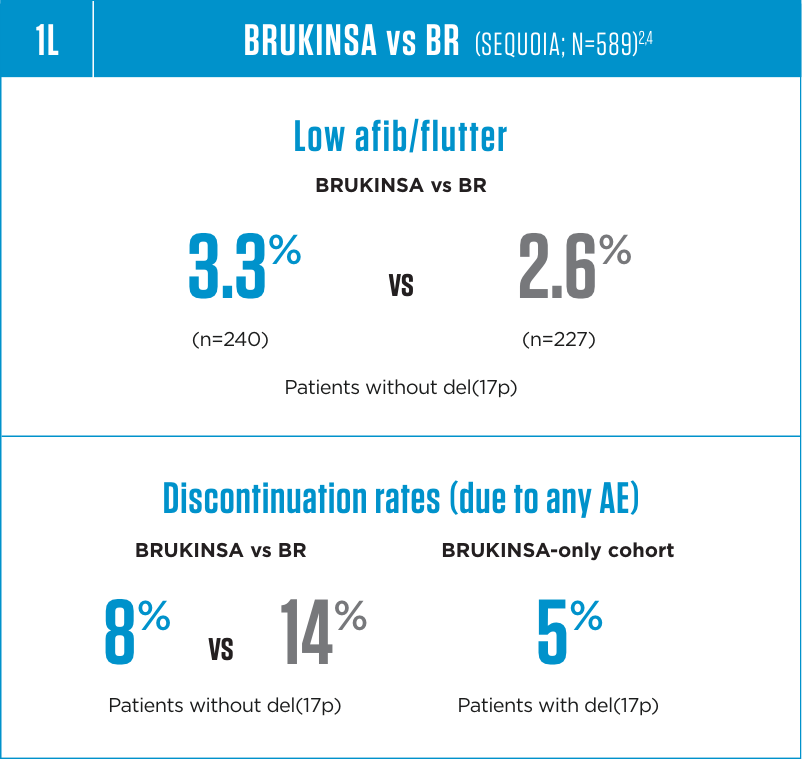
Median duration of treatment: 26.1 months for BRUKINSA and 5.6 months for BR in Cohort 1; 30.0 months for BRUKINSA in Cohort 2.4
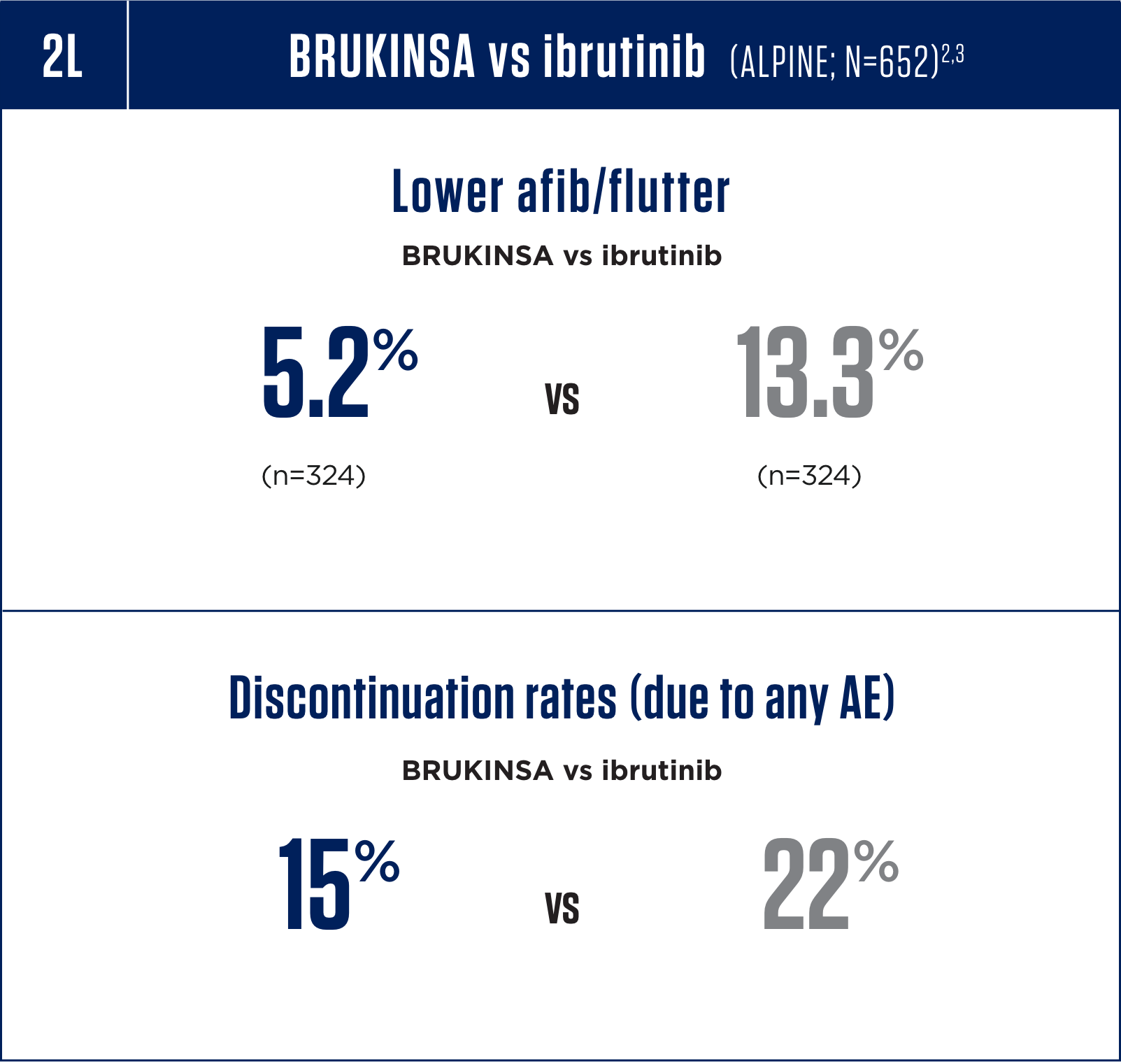
Median duration of treatment: 28.4 months for BRUKINSA and 24.3 months for ibrutinib.3
Serious adverse reactions, including fatal events, have occurred with BRUKINSA, including hemorrhage, infections, cytopenias, second primary malignancies, cardiac arrhythmias, and hepatotoxicity (including drug-induced liver injury). In the pooled safety population (N=1729), the most common adverse reactions (≥30%), including laboratory abnormalities, in patients who received BRUKINSA were neutrophil count decreased (51%), platelet count decreased (41%), upper respiratory tract infection (38%), hemorrhage (32%), and musculoskeletal pain (31%).2
1L=first line; 2L=second line; AE=adverse event; afib=atrial fibrillation; BR=bendamustine+rituximab.
Dr Anthony Nguyen discusses how BRUKINSA has benefited his patients
Zanubrutinib (BRUKINSA®) is a National Comprehensive Cancer Network® (NCCN®) preferred treatment option for patients with CLL8:
Without del(17p)/TP53
First-line: NCCN Category 1
Second-line: NCCN Category 1
With del(17p)/TP53
First-line: NCCN Category 2A
Second-line: NCCN Category 1
Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma V.1.2026. © National Comprehensive Cancer Network, Inc. 2025. All rights reserved. Accessed October 10, 2025. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
Personalized patient support
dedicated to helping eligible patients
A personalized support program designed to help guide and assist patients, caregivers, and practices.
-

Simplifying Access
-

Educating Patients
-

Securing Support
References: 1. Data on file. BeOne Medicines USA, Inc. 2. BRUKINSA. Package insert. BeOne Medicines USA, Inc.; 2025. 3. Brown JR, Eichhorst B, Hillmen P, et al. Zanubrutinib or ibrutinib in relapsed or refractory chronic lymphocytic leukemia. N Engl J Med. 2023;388(4):319-332. 4. Tam CS, Brown JR, Kahl BS, et al. Zanubrutinib versus bendamustine and rituximab in untreated chronic lymphocytic leukaemia and small lymphocytic lymphoma (SEQUOIA): a randomised, controlled, phase 3 trial. Lancet Oncol. 2022;23(8):1031-1043. 5. Tam CS, Munir T, Robak T, et al. Sustained efficacy of zanubrutinib vs bendamustine + rituximab in treatment-naive chronic lymphocytic leukemia/small lymphocytic lymphoma and continued favorable survival in non-randomized patients with del(17p): 6-year follow-up in the phase 3 SEQUOIA study. Presented at: American Society of Hematology (ASH) Annual Meeting and Exposition; December 6-9, 2025. Poster 2129. 6. Brown JR, Eichhorst B, Lamanna N, et al. Sustained benefit of zanubrutinib vs ibrutinib in patients with R/R CLL/SLL: final comparative analysis of ALPINE. Blood. 2024;144(26):2706-2717. 7. Data on file. BeiGene USA, Inc. 8. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma V.1.2026. © National Comprehensive Cancer Network, Inc. 2025. All rights reserved. Accessed October 10, 2025. To view the most recent and complete version of the guideline, go online to NCCN.org.