POWERFUL AND
DURABLE RESPONSES
Adults with WM rapidly achieved high response rates regardless of line of therapy or mutation.
POWERFUL AND CONSISTENT RESPONSES
WITH BRUKINSA ACROSS ALL WM PATIENTS
While the primary endpoint of superiority did not reach statistical significance, numerically higher VGPR rates were achieved in the BRUKINSA treatment arm.1
Initial analysis (19 months)2
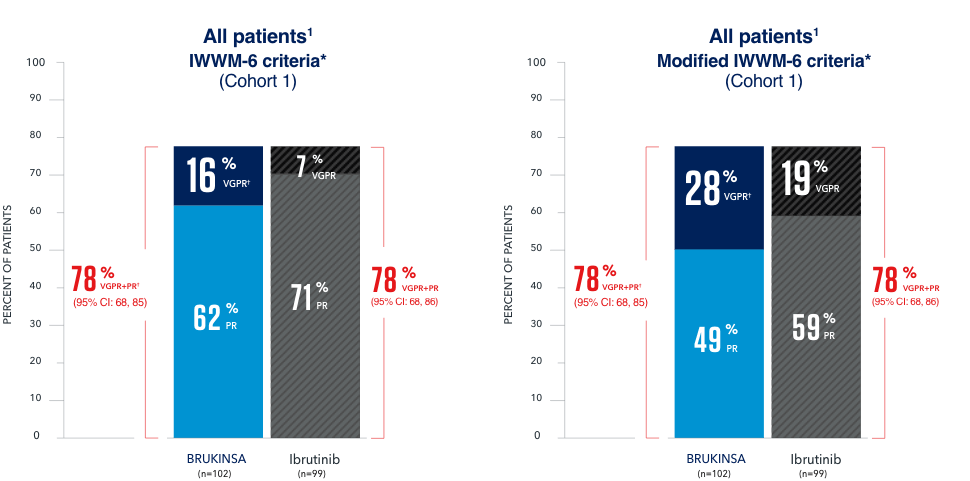
In all patients, median time to response (CR+VGPR+PR) was 2.8 months for the BRUKINSA arm and 2.9 months for the ibrutinib arm.3
The median follow-up time was 19.4 months.2
The prespecified efficacy outcome measure of VGPR/CR was assessed by IRC.1
CONSISTENT RESPONSES WITH BRUKINSA
REGARDLESS OF LINE OF THERAPY
Initial analysis (19 months)2
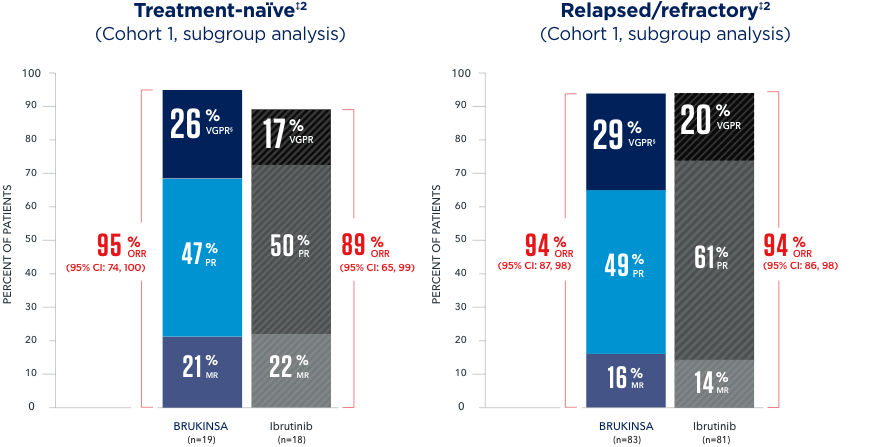
All subgroup analyses are exploratory and descriptive in nature.
The median follow-up time was 19.4 months.2
CONSISTENT RESPONSES WITH BRUKINSA
REGARDLESS OF MUTATION
Initial analysis (19 and 18 months, respectively)2,6
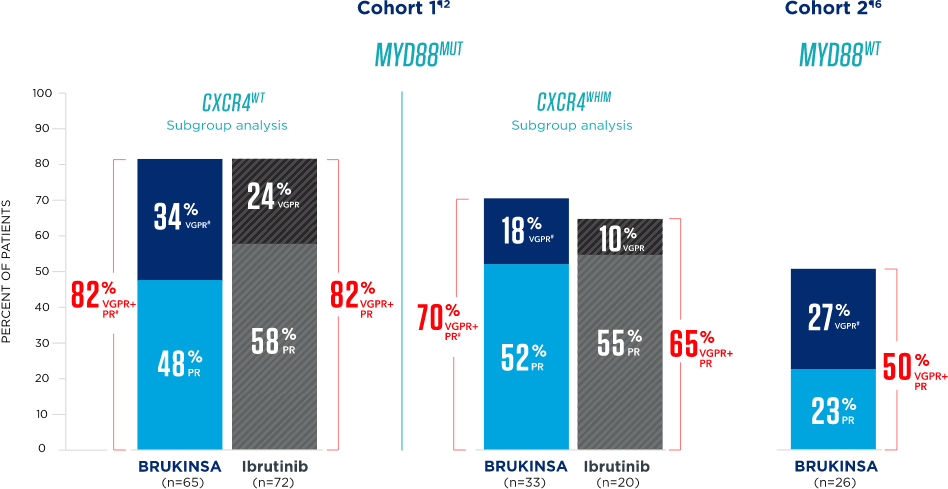
All analyses are exploratory and descriptive in nature.
The median follow-up time was 19.4 months for Cohort 1 and 17.9 months for Cohort 2.2,6
RESPONSES CONTINUED OVER TIME REGARDLESS OF MUTATION
Long-term analysis (44 months and 43 months, respectively)7
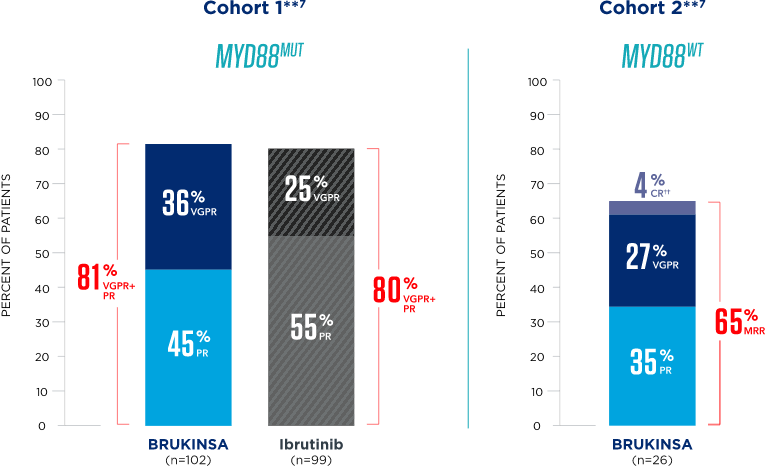
All analyses are exploratory and descriptive in nature.
The median follow-up time was 44.4 months for Cohort 1 and 42.9 months for Cohort 2.7
DURABLE DISEASE CONTROL
WITH BRUKINSA
Sustained responses in patients who achieved a response (CR+VGPR+PR)
Initial analysis (19 months)2
All subgroup analyses are exploratory and descriptive in nature.
Median duration of response (VGPR/CR) was not reached in either treatment arm.2
The median follow-up time was 19.4 months.2
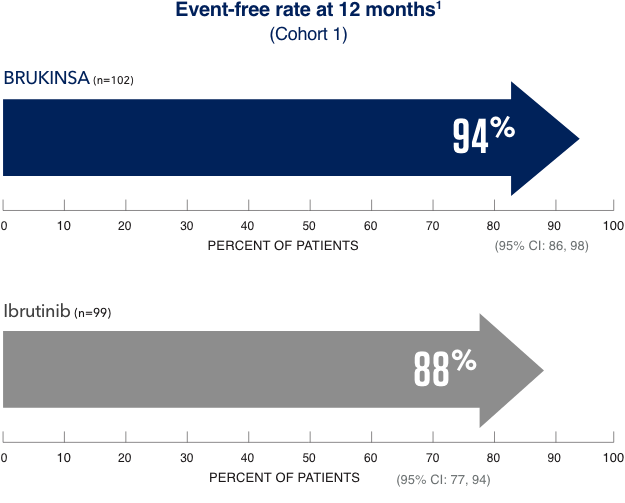
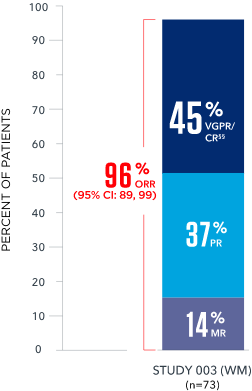
CONSISTENT RESPONSES CONTINUE WITH BRUKINSA
STUDY 003: A PHASE 1/2 SUPPORTIVE STUDY8
A Phase 1/2, open-label, multicenter, single-arm trial including 77 patients with treatment-naïve and relapsed/refractory WM‡‡
Data are consistent with results observed in ASPEN (Study 302) and the overall safety profile of BRUKINSA.8
Median follow-up time was 24 months in patients with treatment-naïve WM and 36 months in patients with R/R WM.8
References: 1. BRUKINSA. Package insert. BeiGene USA, Inc.; 2025. 2. Tam CS, Opat S, D’Sa S, et al. A randomized phase 3 trial of zanubrutinib vs ibrutinib in symptomatic Waldenström macroglobulinemia: the ASPEN study. Blood. 2020;136(18):2038-2050. 3. Data on file. BeiGene USA, Inc. 4. Owen RG, Kyle RA, Stone MJ, et al. Response assessment in Waldenström macroglobulinemia: update from the VIth International Workshop. Br J Haematol. 2013;160(2):171-176. 5. Treon SP. How I treat Waldenström macroglobulinemia. Blood. 2015;126(6):721-732. 6. Dimopoulos M, Sanz RG, Lee HP, et al. Zanubrutinib for the treatment of MYD88 wild-type Waldenström macroglobulinemia: a substudy of the phase 3 ASPEN trial. Blood Adv. 2020;4(23):6009-6018. 7. Tam CS, Garcia-Sanz R, Opat S, et al. ASPEN: long-term follow-up results of a phase 3 randomized trial of zanubrutinib versus ibrutinib in patients with Waldenström macroglobulinemia. Poster presented at: American Society of Clinical Oncology (ASCO) 2022 Annual Meeting; June 3-7, 2022. Abstract 7521. 8. Trotman J, Opat S, Gottlieb D, et al. Zanubrutinib for the treatment of patients with Waldenström macroglobulinemia: 3 years of follow-up. Blood. 2020;136(18):2027-2037.